Salivary Duct | Endoscopic Salivary Surgery | Salivary Gland
Salivary Stones | Stenosis | Parotiditis | Sialadenitis| Strioture |Mucocele | Sialendoscopy
The blockage of salivary flow gives rise to swelling and pain of the gland. Sometimes the pain is quite sudden and feels like a colic. Most often, sudden meal-time swelling is followed by a slow decompression of the gland. Gentle massages over the gland seem to help the process. If bacteria infect the non-moving saliva, then fevers and chills may be present. Pus can be milked from the duct and the gland area is reddish and swollen.
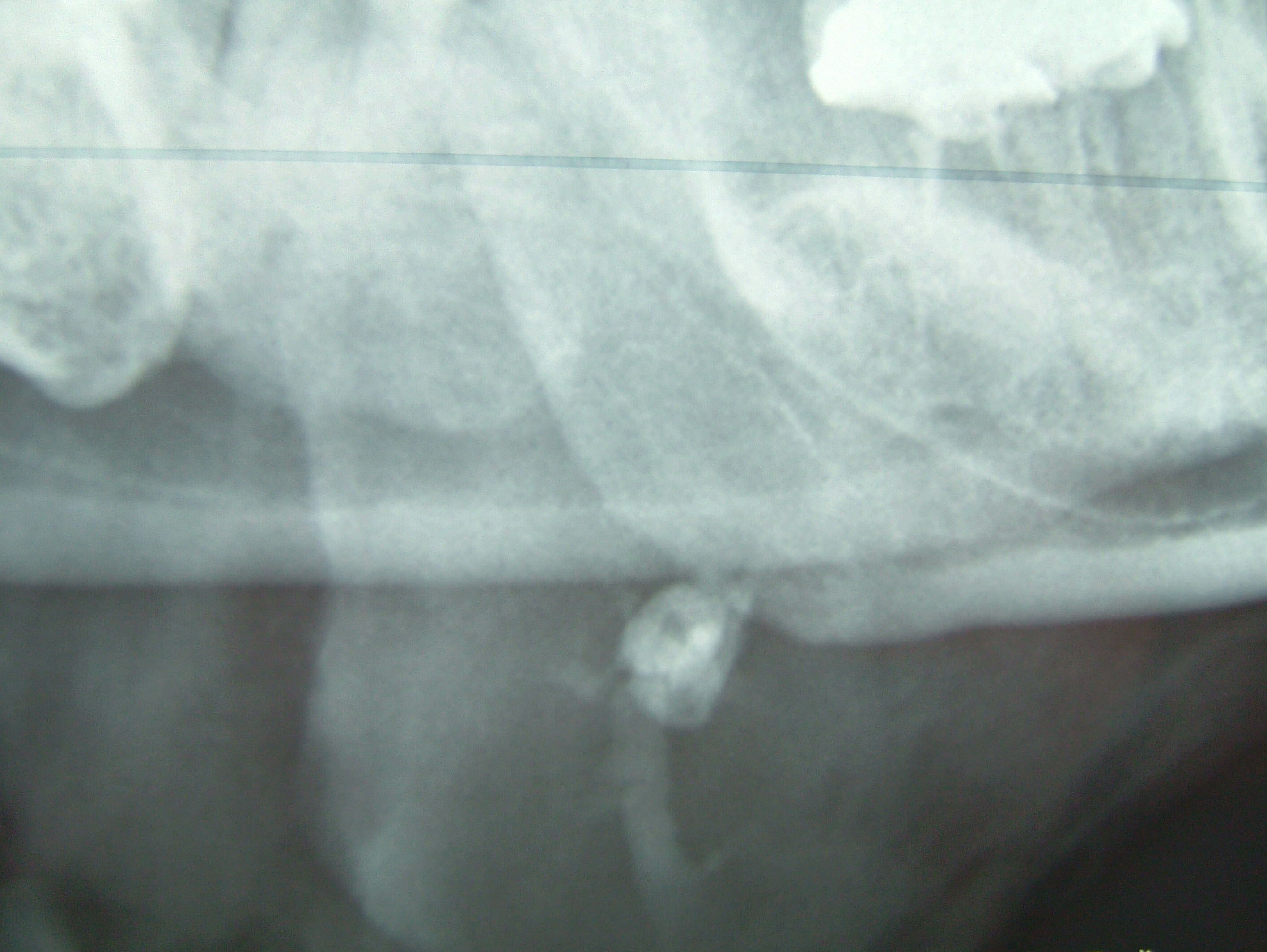
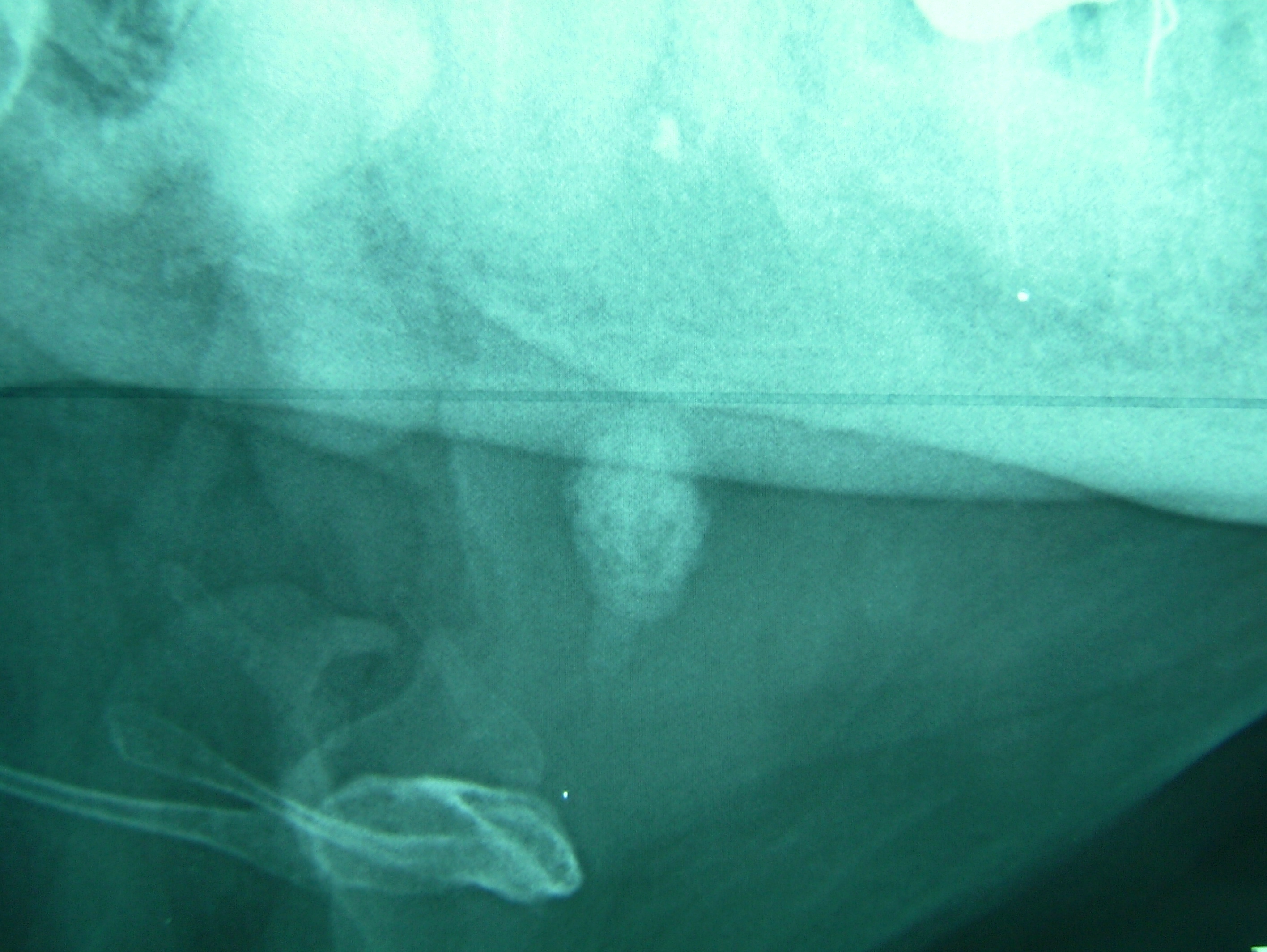
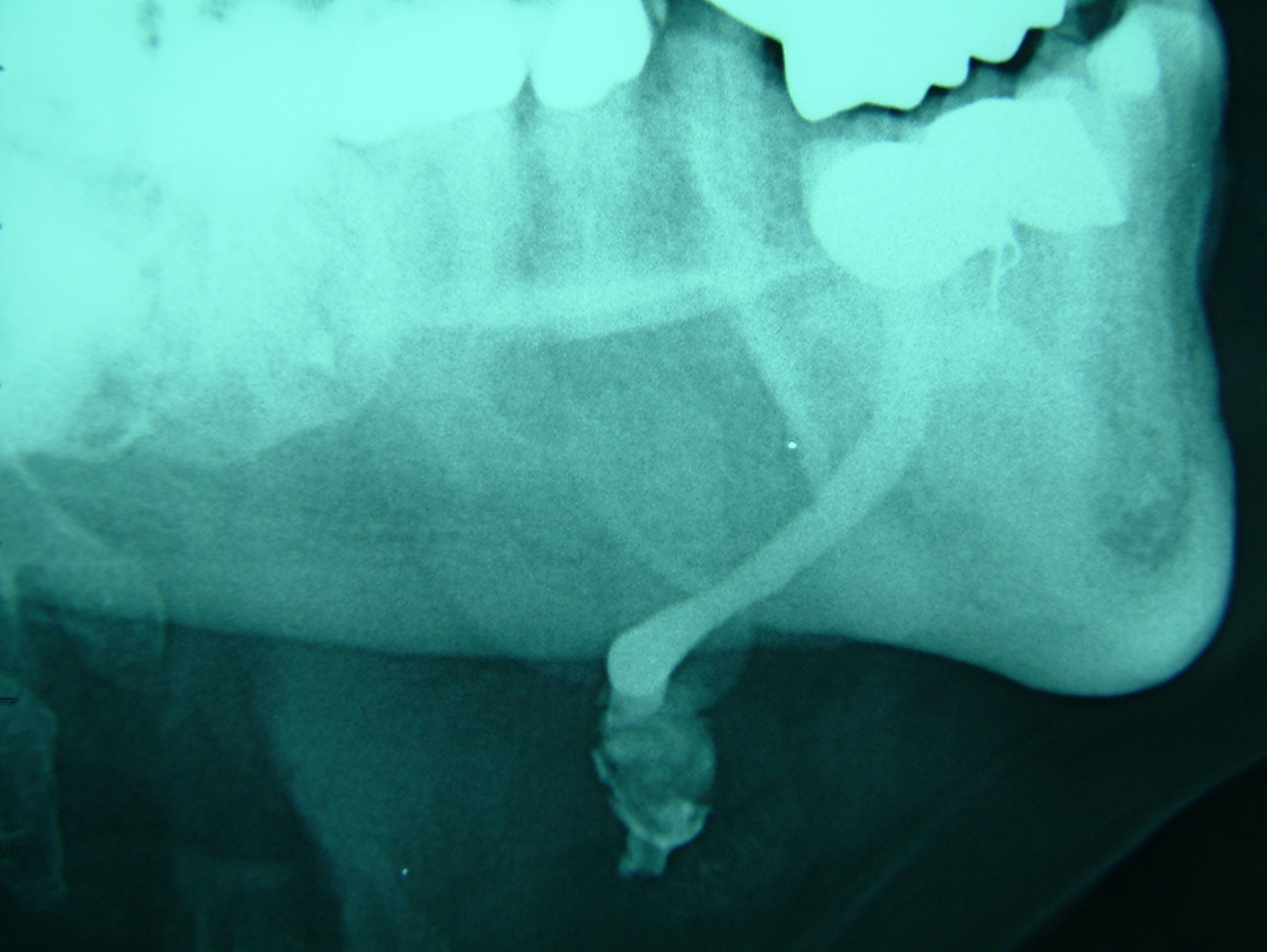
Diagnosis of the condition is made by the history, physical exam, and radiologic imaging. A formal work-up using imaging studies such as sialogram, CT, and MRI scans confirms the diagnosis of stones and rules out tumor and other diagnoses.
Treatment is initially directed to halting any acute infection by the administration of antibiotics and sialograms. If the infection is severe, hospitalization may be necessary for intra-venous treatment. After the acute phase has significantly quieted, then attention can be turned towards the stones and relief of the obstructed duct.
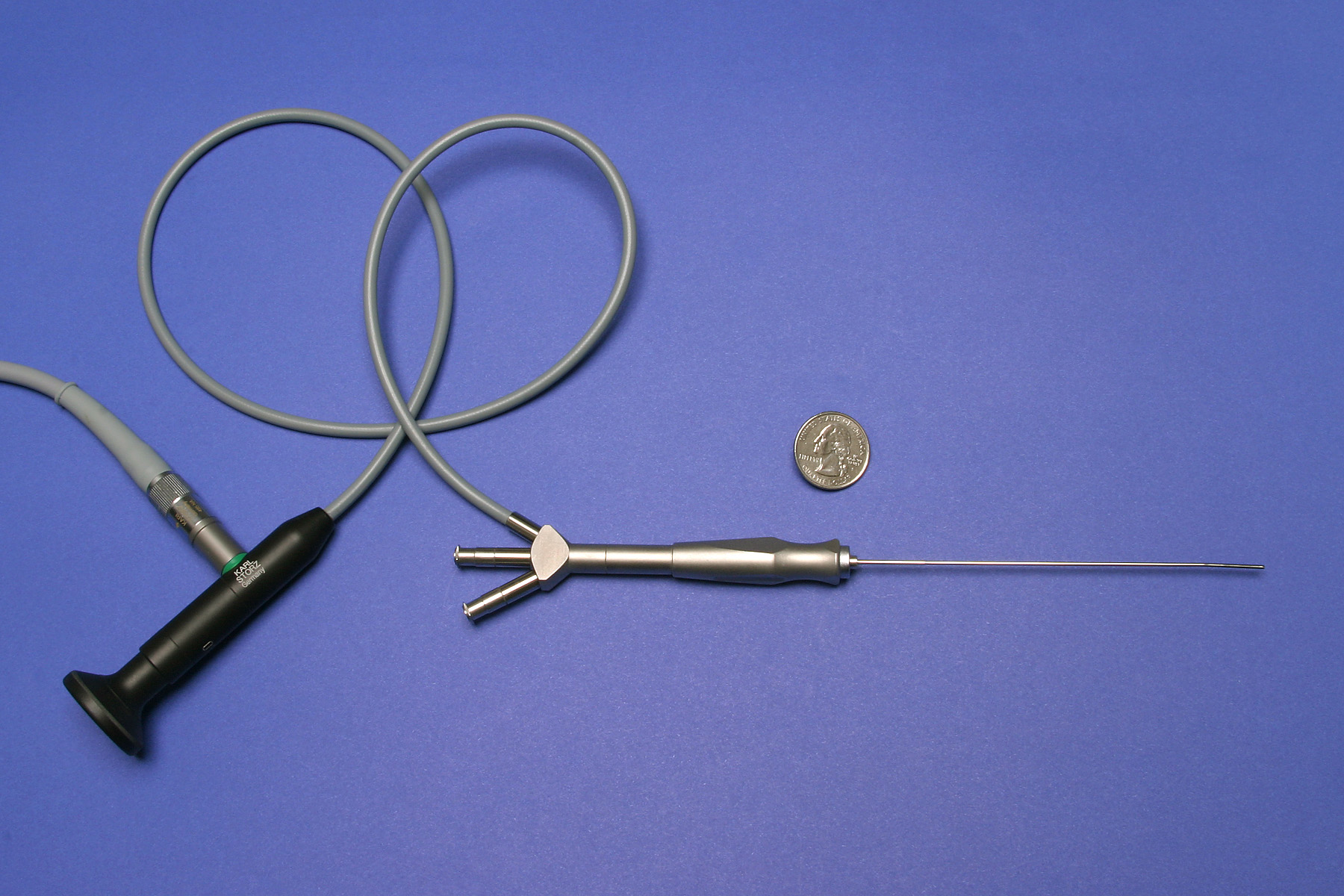
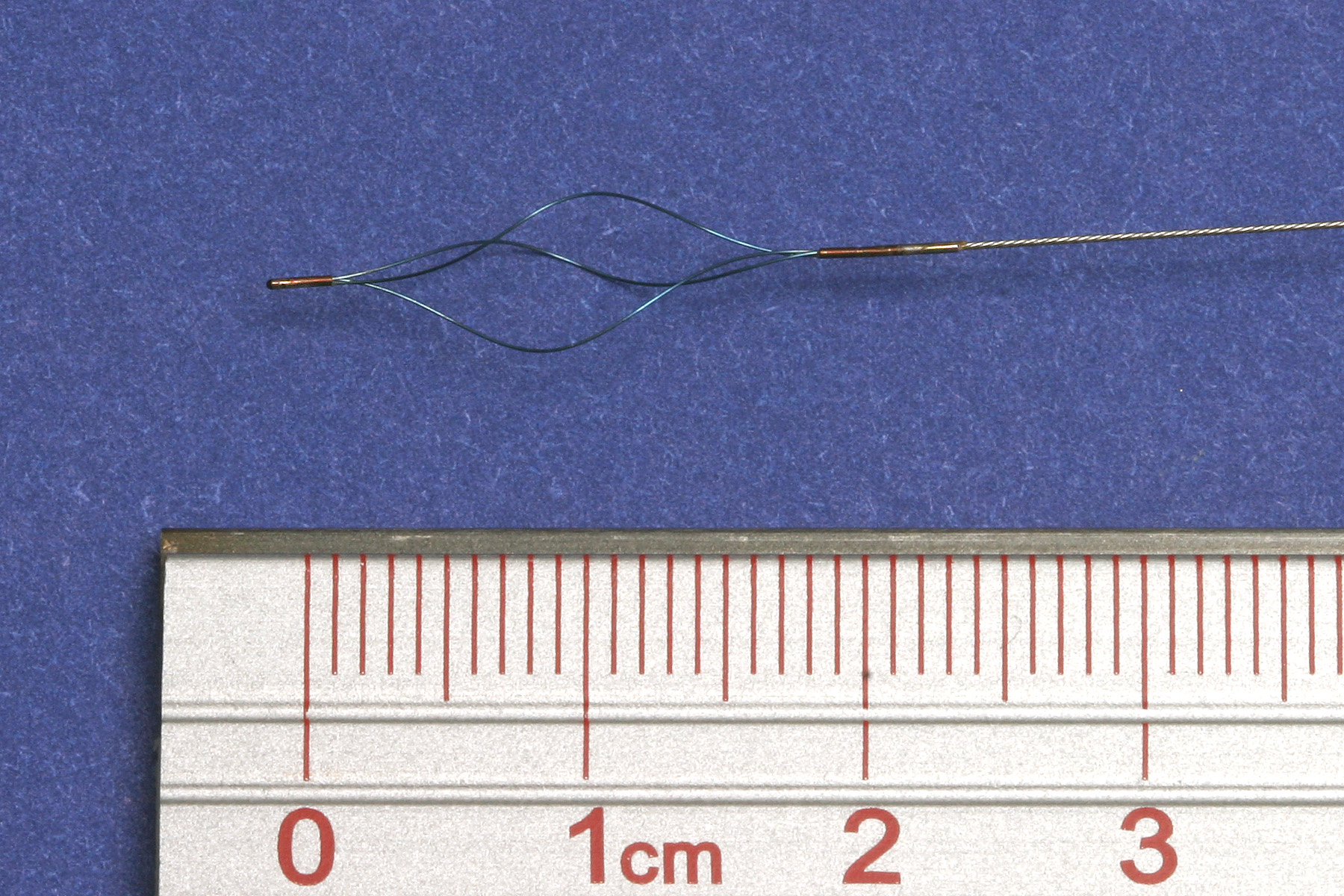
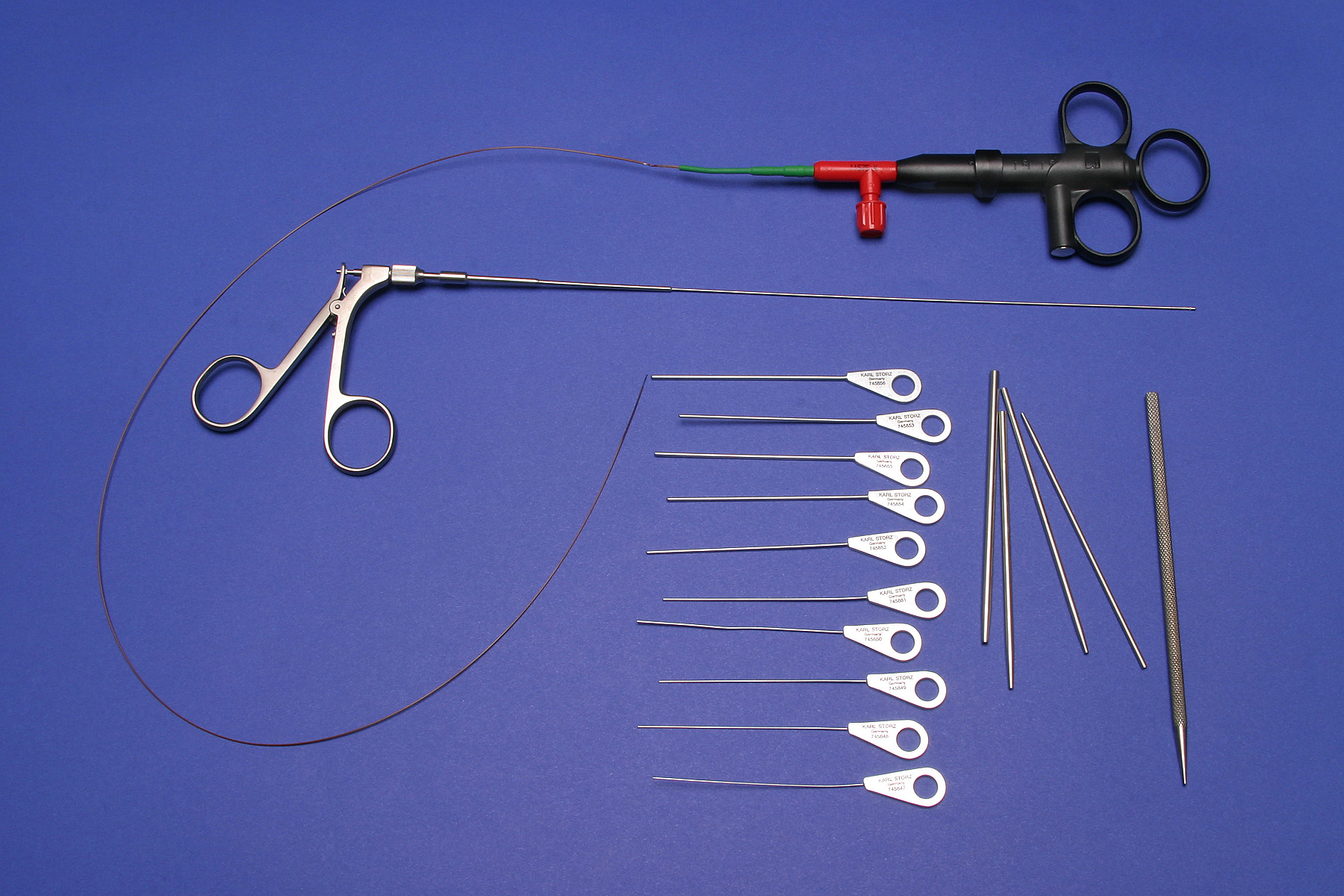
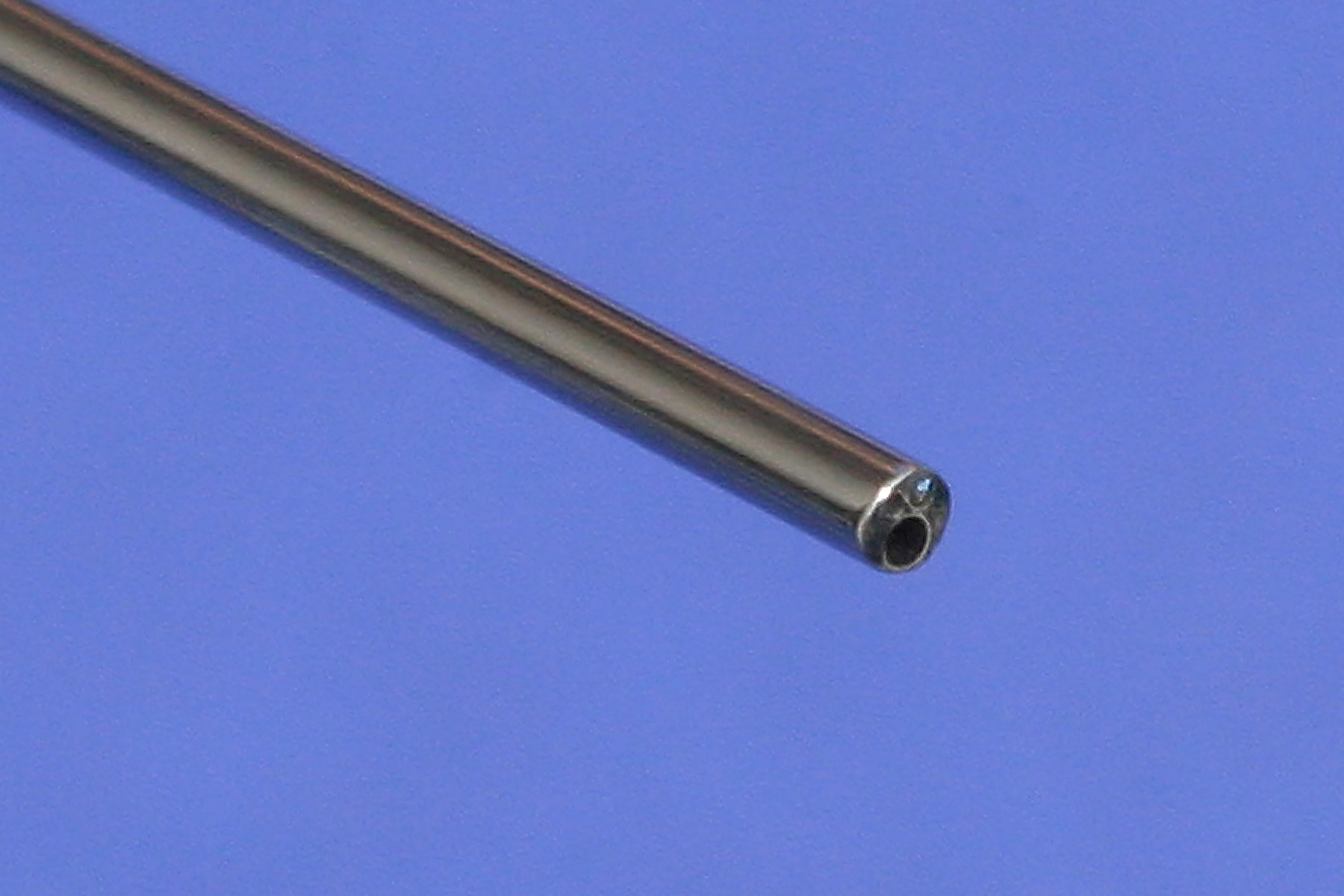
Definitive treatment of the stones is directed at preserving and restoring normal anatomy and physiology to the gland. Direct treatment of the stones involves endoscopy. Endoscopy is a process whereby the surgeon can look into and work on the duct and stones by using a thin, rod-like optical device. The outside diameter of the endoscopes ranges from 1.1 to 1.3 millimeters. The diameter includes optical and working channels. Micro-instruments such as forceps, basket snares, balloon dilators and laser fibers are used through the working channels.
Small stones are removed directly, whereas large stones are first broken into smaller pieces by laser lithotripsy before endoscopic removal. Most stones can be successfully treated by the endoscopic technique. Sometimes overly large or intra-glandular stones or the finding of a salivary gland tumor would require open surgical approaches.
Another problem which causes duct blockage is a tight area of duct known as a “stenosis” or “stricture”. There is a blockage to saliva flow. Fortunately, these can be treated using endoscopy.
The advantage of the endoscopic technique is that the gland can be returned to normal health and function. Also, since all work is done through the patient’s mouth and within the duct itself, no external surgical incisions are needed. The patient is saved the pain and possible complications of open conventional surgery. Most specifically, the risk of a facial nerve paralysis, incision line scar, and the cosmetic concavity of removed gland tissue are avoided. Depending on the stone size and location, either local or general anesthesia is given. An out-patient surgery, or sometimes an overnight stay are usual. Relief is immediate as the offending blocking stones are removed.
External (extra-corporeal lithotripsy) shock wave therapy is not USA FDA approved. Therefore, this treatment is not available in the U.S.A. Lithotripsy clinics usually need multiple sessions with the lithotriptor to make the stones asymptomatic. Usually, there is a 3 week hiatus between sessions to allow the gland and duct to recover.





equipment_photo_2
equipment_photo_1

equipment_photo_7
equipment_photo_6
equipment_photo_5
equipment_photo_4